By  Professor Satya Narayan Misra in Bhubaneswar, April 6, 2026: The establishment of Niti Aayog in 2015 marked a paradigm shift from Nehru-Mahalnobis model of centralised planning to a model of networked, evidence based governance, where it seeks to influence policy through coordinated monitoring and innovation.Professor Satya Narayan Misra in Bhubaneswar, April 6, 2026: The establishment of Niti Aayog in 2015 marked a paradigm shift from Nehru-Mahalnobis model of centralised planning to a model of networked, evidence based governance, where it seeks to influence policy through coordinated monitoring and innovation.
Professor Satya Narayan Misra in Bhubaneswar, April 6, 2026: The establishment of Niti Aayog in 2015 marked a paradigm shift from Nehru-Mahalnobis model of centralised planning to a model of networked, evidence based governance, where it seeks to influence policy through coordinated monitoring and innovation.Professor Satya Narayan Misra in Bhubaneswar, April 6, 2026: The establishment of Niti Aayog in 2015 marked a paradigm shift from Nehru-Mahalnobis model of centralised planning to a model of networked, evidence based governance, where it seeks to influence policy through coordinated monitoring and innovation.
Its flagship program –The Aspirational District Program, provides a useful lens to evaluate this transformation. The introduction of 49 Key Result Areas (KRAS) across five sectors, viz Health & Nutrition, Education, Agriculture & Water Resources, Financial Inclusion & Skill Development & Basic Infrastructure enables granular monitoring of incremental change. Out of 112 districts chosen, Odisha account for 10, which largely belong to the beleaguered K-B_K region of Odisha. The reports highlight that the gains are often concentrated in low hanging fruit indicators, while structural challenges like income generation and employment remain less addressed.
The Major Concerns
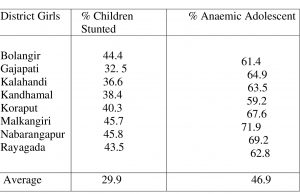
Odisha has been able to scale down its Multi-dimensional poverty % from 29.3% in 2015 to 15.68% by 2023. However serious interdistrict imbalances persist, with Puri achieving 3.3%, while districts like Malkangiri (45%), Koraput (33.4%) and Rayagada (34% seethe with very high numbers. Stunting among children, which is a marker of long term nutrition, & poor sanitation making children prone to frequent infection, is 15% higher in these aspirational districts than average score of all districts, apart from anaemia among adolescent girls which is similarly alarmingly high. The following table, based on NFHS V Survey, will bring out the contrast between these ADs and the average score in terms of stunting & anaemia.
The Mixed Bag
To be fair to the Aspiraional District Program, some of the districts have achieved progress in certain area. For instance, in Rayagada & Kandhamal institutional delivery improved by 20% by converting Sub centres in to Ayushman Arogya Mandir. Basic infrastructure also shows improvement in terms of rural electricity, individual latrines and drinking water under the HarGhar Jal mission.
Road connectivity under the PM GSY has improved access for ambulances in these hilly areas. In the area of educational outcomes, Nuapada district shows improvement, particularly in terms of girl friendly toilet. However, slow or no progress is witnessed in respect of anaemia among women even though IFA (Iron & Folic Acid) distribution has reached 90% saturation level, the actual haemoglobin levels have not risen proportionally. Wasting, a phenomenon where low weight for age is seen shows an uptick in the Malkangiri district.
Besides, in the area of Skill development & financial inclusion, all the ten districts score low delta scores. While the Jan Dhan accounts exist, meaningful usage & insurance penetration is low because of lack of banking correspondents in remote areas. Creating local jobs for tribal youth remains most difficult; most skilled youth still migrate to AP/Telengana for work. For Skill development, the focus must be on local livelihood.
Training on processing forest produce, inculcating modern agri skills like solar pump maintenance, use of drone for pesticide spraying must be given priority. Use of World Skill Centre as a hub to train master trainer – who then run sub centres is critical. The Handloom & Handicraft Cluster should facilitate high end designers to in turn train local weavers. By converging Mission Shakti to NUA Odisha skilling, these districts can move from, ‘aspirational’ to ‘inspirational’.
The Intractable Challenge of Anaemia
Article 47 of our Constitution enjoins upon states to ‘raise the level of nutrition’. Anaemia among women is showing an increasing trend in every state except Kerala as per successive NFHS surveys. In case of Odisha it has climbed up from 51.8% in 1989-99 to 57% in 2019-21. Mrs Gandhi launched the mega ICDS program in 1975 as a comprehensive program to contain the high levels of under nutrition and anaemia among children and expecting and nursing mothers through a slew of Anganwadi centres by providing supplementary nutrition and iron folic acid supplementation.
The NIP (2013) targeted reduction of anaemia by 18% by 2020. It ironically witnessed an increase in anaemia by 3% in 2021. Modi launched the Poshan program in 2018 with an avowed objective of reducing anaemia by 3% per year. Mr Naveen Patnaik, launched the AMLAN program in Odisha in 2022. However, as already brought out, the trend has neither been reversed nor contained in most states, including Odisha.
Primary Causes of High Anaemia among Adolescent Girls
 Adolescence is a period of rapid physical growth and sexual maturation. The onset of monsoon signal increases the daily requirement of iron to replace blood loss. In case of tribals, their diets lack diversity as they rely on monotonous cereal based diet that is low in iron & Vitamin C, which is essential for iron absorption. To complicate matters, they are afflicted by genetic factors like high presence of Sickle Cell disease. In case of Bolangir & Kalahandi, many carry sickle cell traits, where standard iron tablets do not cure this type of anaemia. Districts like Koraput & Malkangiri suffer from 70% anaemia due to high malarial endemicity.
Adolescence is a period of rapid physical growth and sexual maturation. The onset of monsoon signal increases the daily requirement of iron to replace blood loss. In case of tribals, their diets lack diversity as they rely on monotonous cereal based diet that is low in iron & Vitamin C, which is essential for iron absorption. To complicate matters, they are afflicted by genetic factors like high presence of Sickle Cell disease. In case of Bolangir & Kalahandi, many carry sickle cell traits, where standard iron tablets do not cure this type of anaemia. Districts like Koraput & Malkangiri suffer from 70% anaemia due to high malarial endemicity.
Low Hanging Fruit Syndrome
It is easy to build a school toilet or provide electricity to a village than to change the eating habits. There is also an accountability gap as they are transferred every 12-18 months. They are incentivised to focus on visible projects rather than invisible nutritional improvements. There is also a disconnect in the convergence strategy of health department with education and WCD departments. There is a gap between IFA tablet distribution and anaemia reduction. Districts like Malkangiri often have 30-40% vacancy in respect of Auxillary Nurse Midwives & ICDS supervisors. One of the suggestions offered is to financially incentivise Asha workers. But they are a partial bridge rather than a complete solution. While the Asha worker get paid for distribution of IFA tablets but are not accountable for ensuring their consumption.
Financial incentives are the fuel but government accountability is the steering wheel. We cannot reach the destination of anaemia free districts without a steering wheel, proper monitoring & departmental convergence. Skill development & financial inclusion must be given highest priority as all the aspirational districts of Odisha are showing persistent deficits.

Leave a Reply
Be the First to Comment!